Volume: 3 Issue: 1
Breast Adenocarcinoma Metastasis Presenting as a Temporal Bone Lesion: Case Report and Review of Literature
Year: 2026, Page: 28-32, Doi: https://doi.org/10.71325/ajjms.v3i1.26.8
Received: Jan. 28, 2026 Accepted: Feb. 9, 2026 Published: May 13, 2026
Abstract
Metastatic involvement of the temporal bone is a rare but clinically significant manifestation of advanced malignancies. Among solid tumors, breast carcinoma is a recognized primary source for temporal bone metastasis, often presenting with otologic or neurologic symptoms. We report a 61-year-old woman with rheumatoid arthritis who experienced sudden onset left lower motor neuron facial palsy. Imaging showed that the left temporal bone had lytic lesions. The facial nerve canal and its surrounding structures were being eroded by a friable tumor that was discovered during surgical examination. The metastatic adenocarcinoma of breast origin was verified by histopathological and immunohistochemical studies. With extensive skeletal metastases, a primary right retroareolar breast tumor was further identified by whole-body PET-CT. This case highlights the importance of considering metastatic disease in patients presenting with atypical facial palsy and temporal bone lesions. Early imaging and histopathological diagnosis are crucial for appropriate oncologic management and prognosis.
Keywords: Metastatic temporal bone lesion; Breast carcinoma; Facial nerve palsy; Adenocarcinoma; PET-CT; Histopathology
INTRODUCTION
Metastasis to the temporal bone is an infrequent clinical entity, often associated with advanced malignancy. The most commonly implicated primary sites include breast, lung, prostate, and renal carcinomas. Due to its rarity and the non-specific nature of symptoms, temporal bone metastasis is frequently misdiagnosed or overlooked during initial evaluation. Patients may present with signs mimicking benign otologic conditions such as chronic otitis media, facial nerve dysfunction, hearing loss, or vertigo.
Among these, facial nerve palsy, persistent otorrhea, and sensorineural hearing loss are notable indicators but are rarely immediately linked to metastatic disease. Temporal bone involvement as the first clinical sign of an undiagnosed systemic malignancy is particularly uncommon and presents a significant diagnostic challenge.
This case report discusses an unusual presentation of metastatic breast adenocarcinoma manifesting primarily with facial nerve palsy and mimicking a benign otologic disorder, ultimately leading to the diagnosis of advanced systemic malignancy.
CASE PRESENTATION
A 61-year-old female, known case of rheumatoid arthritis, presented with sudden-onset left-sided lower motor neuron facial palsy of 20 days duration. She also reported a history of intermittent back and joint pain over the preceding months. Initial management included low-dose corticosteroids, which were later escalated to high-dose steroids due to lack of clinical improvement. Despite this, there was no resolution of facial weakness.
As symptoms persisted, an MRI of the brain and temporal bone was performed, which revealed lytic lesions involving the left mastoid and petrous temporal bone. In view of these findings and the progressive nature of the facial palsy, the patient underwent an emergency mastoid exploration under general anesthesia.
Intraoperatively, a pale pink, friable proliferative mass was found occupying the mastoid cavity, with erosion of the dural plate, ossicles, and facial nerve canal, and extension toward the petrous apex. Complete excision was not feasible due to proximity to critical neurovascular structures; however, maximum debulking was performed. Conchomeatoplasty was carried out, and biopsy specimens were sent for histopathological evaluation. A second-stage surgery was planned for hearing reconstruction.
Histopathology revealed a poorly differentiated adenocarcinoma, and immunohistochemistry confirmed it to be of breast origin. Subsequently, a whole-body PET-CT was performed to locate the primary and assess the metastatic burden. The scan showed an FDG-avid, heterogeneously enhancing, lobulated lesion in the retroareolar region of the right breast, measuring 4.4 × 3.4 × 5.1 cm, with central skin infiltration. Additional findings included:
-
Non-FDG avid satellite nodules surrounding the primary lesion.
-
FDG-avid cutaneous nodules in the right breast.
-
Right axillary Level I lymphadenopathy (largest node 1.5 × 1.4 cm).
-
No significant supraclavicular or internal mammary involvement.
-
A single faintly FDG-avid pulmonary nodule (7.5 mm, SUVmax 1.3) in the left lung.
-
Multiple lytic and sclerotic lesions involving the left temporal bone, right mandible, humeral head, scapula, sternum, spine, pelvic bones, and femurs, with the highest FDG uptake (SUVmax 7.4) noted in the left sacral wing.

Fig. 1: Patient presenting with Bell’s palsy
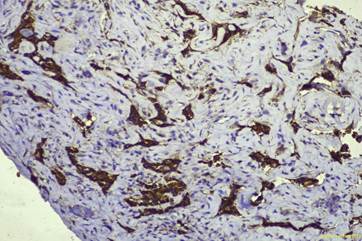
Fig. 2: immunohistochemistry findings-Tumour cells express CK, CK7, and GATA3. Very focal positive to P40. Negative to CK20, TTF1, P63, and Napsin A
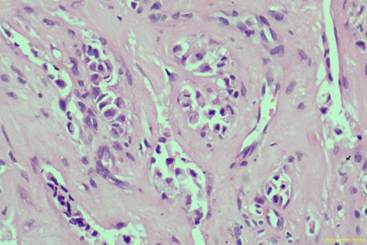
Fig. 3: histopathology showing features suggestive of poorly differentiated adenocarcinoma with numerous signet ring-like cells
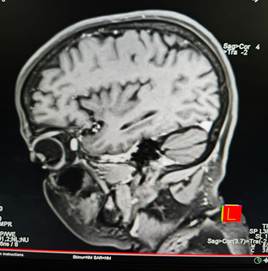
Fig. 4: MRI brain showing lytic lesions in the mastoid
DISCUSSION
Temporal bone metastasis is an uncommon but clinically significant manifestation of systemic malignancies. Breast cancer is among the most frequent primary tumors to metastasize to the temporal bone, along with lung, kidney, and prostate carcinomas [1, 2, 6]. The temporal bone’s rich vascularity and complex anatomical structures make it a potential site for metastatic seeding, often mimicking benign otologic conditions such as chronic otitis media or Bell’s palsy [5, 6].
In this case, the patient's initial presentation with isolated facial nerve palsy is consistent with prior reports indicating that facial nerve involvement is a common early symptom of temporal bone metastasis [2, 6, 8]. The absence of otologic complaints can delay diagnosis, emphasizing the importance of imaging when facial palsy is unresponsive to standard therapy. MRI remains a cornerstone for identifying soft tissue lesions and bony erosion, while PET-CT plays a pivotal role in assessing the primary site and extent of systemic metastases [10].
Histologically, metastatic adenocarcinomas are often poorly differentiated, requiring immunohistochemical staining to confirm tissue of origin, as demonstrated in this patient. Literature indicates that breast cancer frequently metastasizes to the petrous apex and internal auditory canal, with erosion of adjacent structures [3, 4, 8]. In our patient, involvement of the mastoid, dural plate, ossicles, and facial canal highlights the aggressive nature of the disease.
The differential diagnosis of destructive temporal bone lesions should include primary temporal bone malignancies, metastatic disease, and granulomatous conditions [1, 6]. Among metastases, adenocarcinoma is the most common histological subtype encountered in the temporal bone [9]. Studies also suggest that PET/CT has higher sensitivity than conventional imaging in detecting early osseous metastases and guiding management [10].
Surgical intervention in such cases is often limited to biopsy or debulking for diagnostic and palliative purposes, given the proximity to critical neurovascular structures and the disseminated nature of disease. Definitive management typically involves systemic therapy tailored to the primary tumor and extent of metastasis [4, 6].
This case reinforces the need for a high index of suspicion for metastatic disease in patients with atypical or treatment-resistant facial palsy. Early identification and multidisciplinary management are essential to optimize patient outcomes.
REVIEW OF LITERATURE
Metastatic involvement of the temporal bone is an infrequent clinical finding and is more often identified during post-mortem evaluations in patients with advanced-stage malignancies. Among various primary cancers, breast carcinoma is recognized as the most common source of temporal bone metastasis in female patients. The clinical presentation is typically nonspecific, with symptoms such as facial nerve palsy, chronic ear discharge, hearing loss, and vertigo. These symptoms can closely mimic benign middle ear diseases, often leading to misdiagnosis and delays in appropriate management.
Several reports have highlighted the diagnostic challenges in such cases. In a case by Lee et al. (2019), a patient with no known history of malignancy presented with otologic symptoms that initially suggested chronic ear disease. Only after surgical intervention and subsequent PET-CT imaging was a diagnosis of metastatic breast carcinoma to the temporal bone established. Similar diagnostic pitfalls have been reported by Chang et al. (2014) and Keles et al. (2011), who described patients with prolonged ear symptoms that were eventually identified as secondary tumors after intraoperative tissue sampling and histopathology confirmed adenocarcinoma.
Yeh et al. (2009) conducted a case series analysis and found that temporal bone metastases commonly present with ambiguous symptoms, often mimicking chronic otitis media or other inflammatory conditions. They emphasized the need for early histopathological examination, particularly when patients do not respond to conventional therapy. Immunohistochemical studies, as noted by Saito et al. (2019), play a pivotal role in identifying the origin of metastatic adenocarcinoma, particularly when the primary tumor is unknown at presentation.
| Author & Year | Primary Site | Presentation | Diagnostic Modality | Key Findings |
|---|---|---|---|---|
| Lee, et al., 2019 [4] | Breast | Facial palsy, otorrhea | Histopathology, PET-CT | Temporal bone metastasis as initial sign of breast carcinoma |
| Chang, et al., 2014 [5] | Breast | Otitis media-like symptoms | Imaging, Biopsy | Mimicked chronic otitis media; intraoperative biopsy led to diagnosis |
| Yeh, et al., 2009 [3] | Breast | Hearing loss, vertigo, facial palsy | HRCT, Histopathology | Nonspecific otologic symptoms delayed diagnosis |
| Keles, et al., 2011 [10] | Breast | Mimicked chronic otitis media | Surgery, Histopathology | Reinforced need for biopsy in atypical otitis media presentations |
| Ianniello, et al., 2017 [7] | Various | Skull base pain, cranial neuropathies | MRI, PET-CT | Described imaging features of skull base metastases |
| Saito, et al., 2019 [6] | Multiple | Otologic symptoms with known malignancy | Histopathology, IHC | Importance of immunohistochemistry in identifying metastatic adenocarcinoma |
| Lee, et al., 2021 [11] | Breast | Systemic metastasis | PET/CT | PET/CT essential in detecting occult primary and bone spread |
| Head Neck Pathol, 2009, 2017 [3, 7] | Breast, Lung, Others | Deafness, otalgia, cranial nerve palsy | Histopathology | Emphasized histologic variants and diagnostic role of tissue biopsy |
Table 1: Comparative Analysis of Published Literature on Temporal Bone Metastases
Advanced imaging modalities contribute significantly to diagnosis and staging. Ianniello et al. (2017) discussed the utility of MRI and CT in delineating bony involvement, while Lee YJ et al. (2021) underscored the superiority of PET/CT in detecting metastatic spread and locating occult primaries. This is especially important in patients where temporal bone metastasis is the initial clinical presentation, as was the case in our patient.
Given the complex anatomy of the temporal bone and its proximity to critical neurovascular structures, complete surgical excision is often not feasible. However, exploratory surgery and targeted biopsy remain essential when clinical suspicion is high, especially in the presence of cranial nerve deficits or symptoms unresponsive to standard treatment. Prompt histopathological diagnosis enables early systemic evaluation and facilitates initiation of appropriate oncologic management.
CONCLUSION
Temporal bone metastasis, though rare, should be considered in the differential diagnosis when patients present with atypical or persistent otologic symptoms—especially facial nerve palsy, chronic otorrhea, and hearing loss unresponsive to conventional therapy. This case underscores the diagnostic challenges posed by such presentations and highlights the importance of maintaining a high index of suspicion, even in the absence of a known primary malignancy. Surgical exploration and histopathological evaluation, including immunohistochemistry, are vital for accurate diagnosis. Early identification facilitates prompt oncologic intervention and may significantly impact prognosis. This case further illustrates that metastasis to the temporal bone can be the first indication of an undiagnosed systemic malignancy such as breast carcinoma.
References
1. Batsakis JG. Tumors of the Head and Neck: Clinical and Pathological Considerations. 2nd ed. Williams & Wilkins; 1979.
2. Manolidis S, Shohet JA, Jackson CG, Glasscock ME. Malignant Glomus Tumors. The Laryngoscope. 1999; 109 (1). Available from: https://doi.org/10.1097/00005537-199901000-00007
3. Choi SH, Park IS, Kim YB, Hong SM. Unusual Presentation of a Metastatic Tumor to the Temporal Bone: Severe Otalgia and Facial Paralysis. Korean Journal of Audiology. 2014; 18 (1). Available from: https://doi.org/10.7874/kja.2014.18.1.34
4. Lee JH, Cho HH, Lee KY. Temporal bone metastasis as the first manifestation of breast cancer. The Journal of International Advanced Otology. 2019;15(1):177–180.
5. Keles E et al. Temporal bone metastasis mimicking chronic otitis media: a case report. Kulak Burun Bogaz Ihtis Derg. 2011;21(1):47–50.
6. Paparella MM . Temporal bone metastases. Paparella’s Otolaryngology, 4th ed. Philadelphia: Saunders; 2003.
7. Ianniello F et al., Skull base metastasis: clinical and radiological findings in 20 patients. Head and Neck Pathology. 2017;11:306–313.
8. Yeh S et al., Breast cancer metastasis to the temporal bone: a case report and literature review. Head and Neck Pathology. 2009;3:217–224.
9. Nelson EG, Hinojosa R. Histopathology of Metastatic Temporal Bone Tumors. Archives of Otolaryngology - Head and Neck Surgery. 1991; 117 (2). Available from: https://doi.org/10.1001/archotol.1991.01870140077010
10. Lee YJ et al., The role of PET/CT in detection of metastatic breast cancer. <I>Cancers (Basel). 2021;13(24):6335.
Copyright
© 2026 Published by Laxmi Memorial Education Trust. This is an open-access article under CC BY 4.0 license. (https://creativecommons.org/licenses/by/4.0/)
Cite this article
Trishika Shetty, Mahesh Santharaya, Pallavi Pavithran, Vishwas K Pai. Breast Adenocarcinoma Metastasis Presenting as a Temporal Bone Lesion: Case Report and Review of Literature. AJ J Med Sci 2026;3(1):28-32